
The home care service of our association arises before the need not covered by public services (following the tradition of marginalization of mental health, mainly because they cannot be easy sellers of their workforce) of care for people with schizophrenia whose lack of awareness of the disease, or as a consequence of their own symptoms, refuse to take medication (protection factor) and / or have a very low level of activity. In these circumstances, attendance at a center is very unlikely, so it was decided to establish the SAD.
Keep reading this article from PsicologíaOnline, if you want to know more about the Cognitive Therapy in a Home Care Service.
Index
- Introduction to cognitive therapy
- The way of understanding the human being
- Cognitive therapy in special circumstances
- Demand and down payment
- Resistance to treatment
- Activity
- Hallucinations and delusions
- Depression
- Anxiety
- Aggressiveness
- Obsessions and compulsions
- Family intervention
- A few notes on substance use
- Therapy for therapists
Introduction to cognitive therapy.
On the other hand, with patients who are attracted to the Center and those who request it, we also do group therapy, which includes, as far as I am concerned, intervention in emotional self-management (in other places called "self-control", with less fortune) and self-esteem (which I preferred to rename "self-acceptance and self-esteem"). I will count how cognitive therapy is useful in each symptom (treated individually or collectively). To finish the general brushstrokes of the activity in the SAD, note that we have the pleasure of collaborating as an internship center with the Master of Clinical Psychology of the UCM. The possibility of capturing and modifying constructions of some of our students has allowed me to include one last point intended for them.
The way of understanding the human being.
My way of working is based on the idea that people are not so disturbed by the facts as by the vision they have of them. Although this is shared by several cognitive therapies, I bet on a constructivist epistemology that assumes the following points:
- Knowledge is "artificial" in nature: it is not a direct representation of reality in itself (objectivism) but a construction of the experience and activity of the subject. From this point of view, the human being, when knowing, does not handle objective data but interpretations of reality, does not discover something that is already there and that before went unnoticed, but his activity as a connoisseur is properly that of inventing a framework through which to give meaning - to be able to interpret - the facts.
- Is contemplated knowledge as an adaptive and evolutionary activity. The human being makes theories and hypotheses about reality, tries to anticipate in some way what is going to happen, to give himself an explanation about the events that happen to him. To the extent that these hypotheses serve to explain their reality, they will be maintained and when they are not explanatory or predictive, they will be invalidated. That is, our beliefs are subjected to a continuous process of revision or "selection by experience" so that they "survive" those of our personal theories that do not receive an invalidation by the experience environment, that is, those that are viable. The objectivist idea of knowledge as a progressive approach -through accumulation of objective data- to the truth is rejected. There is no true but viable knowledge.
- To know is to grasp a difference. According to this principle we do not know by capturing the inherent properties of an essential reality, that is, we do not carry out a process of abstraction of what is defining or essential in a reality or object, this is knowledge conceptual. Our knowledge is organized around constructs that, as the name itself indicates, are not abstract representations that reflect reality, but ways of constructing it by establishing differences. Knowledge is something relational based on the establishment of a set of identifications and differences between the objects of what we call the real world.
- The knower and the known are inseparable. Independence and dualism between subject and object are rejected as positivism intended, since a true interaction is established between the two.
- Language is the artifact par excellence to carry out knowledge and the construction of the "real". It is not a mediational variable that conditions us in some way when approaching "external reality" objective and positive, but language delimits our realities, we move in universes linguistic.
The mind is no longer studied as an entity located inside the individual or in his head, we could say that now the mind is "between" the individuals and thus, it is analyzed insofar as it represents an action on the surrounding environment, therefore, with an instrumental value. But at the same time, this mind and all higher mental functions, being socially mediated, will have cultural meanings and they will play a role in the social life of the community, that is, mental activity is no longer seen as something private or individual, but as activity with social meaning.
This finds its reflection in the psychological theory of constructionism in the idea that social groups (societies, communities, families ...) develop "dominant narratives", this It is, hegemonic forms of explanation of reality that are shared by its members and that refer to a mode of lifetime. From the constructionist perspective, such dominant narratives can in many cases be at the origin of emotional maladjustments (p. Eg Narrations in which the value of the person depends on the successes he achieves, the meaning of life depends on the approval of others or the "hero" is the most competitive person).
I would like to review the importance that economic and social conditioning produces in the functioning of the conscience of the individual and specifically in the conscience of a subject with schizophrenia, so that no Let's lose the perspective that these individual or group interventions are nothing more than mere patches (exciting, useful, even commendable) under conditions that are beyond the power of the therapist and, under other circumstances, would make him lose (fortunately) a large amount of job. A Warner study, frequently cited by Max Birchwood and Filiberto Fuentenebro (from Birmingham and Madrid, respectively), for example, alleges that recovery rates from The introduction of antipsychotic drugs are not superior to those immediately after the Second World War, but it does appear that the rates decreased during the great depression. During the great depression of the 1920s and 1930s, complete recovery dropped to 12% and social recovery to 29% Birchwood adds (I had the chance to hear him say about a year ago) that the number of cases in Britain of second-generation blacks is five times higher. It's food for thought, right?
To conclude this introduction, it is essential to note the improvements that cognitive therapy has been trying for a few years include: a new concept of therapeutic relationship in which the patient is no longer judged based on whether the information is processed poorly or well, if distorts or not, but in which the realities are multiple (as Watzlavick says) or at least they are created and transformed at the same time assimilate; include the importance of the non-conscious (eg, non-conscious schemas or algorithms) to understand conscious processes and outcomes. Focus more on non-verbal information, not propositional but implicational; the emotional fixed point of Wessler's Cognitive Appraisal Therapy or the downward arrow technique, for which it takes a good dose of intuition or having experienced the role of patient (FEAP recommendation), which show. Focus more on the role of emotion and its expression (hence the tendency to dispense with the concept of self-control) as we can find in therapies dedicated to cases of post-traumatic stress disorder or schema-focused cognitive therapy, in which child schema formation with emotional information plays a crucial role associated.
All this, after all, to achieve optimal results in psychotherapy, that art of mixing different elements and where, as in alchemy, excellence is sought, the transformation of an ordinary metal into gold (Isabel Caro).
Cognitive therapy in special circumstances.
The quintessential technique in cognitive therapy is debate, in order to build a new narrative with which to tell the events that happened. I assume at this point a posttrationalist nuance (although not postmodernist, since reason, from my point of view, already makes a crisis in dialectics), since it is each It is increasingly difficult to refute those who affirm that we therapists are not objective judges who distinguish between the error and the success of the patient when processing, but that we propose to modify the interpretation of reality based on an element (language) that by necessity is going to be fragmentary where reality does not it is. These events can be psychosocial micro-stressors, depresogenic or anxiogenic events, disruptive behaviors of a family member, events that trigger delusions... and (attention!) your own hallucinations and obsessions or impulses.
Therefore, it is easy to imagine that, no matter how much you want it, the systematicity in each area to intervene and every moment of the therapeutic process it will not be similar. I mean that we can get from a quasi-informal dialogue while walking the patient's dog next to him, to the systematicity of:
- link the original narrative with possible distortions,
- with dominant narratives in the culture,
- questions to expand information and search for new meanings,
- constructs that are applied in that narrative and escalations,
- moments in the past when they were applied
- and elicitation of a new, more adaptive narrative with which to describe the event.

Demand and down payment.
Let's keep in mind that the request has been made by a third person. The family member arrives at our service without having discussed it with the patient. We are then in a situation in which we border on what is ethically acceptable. In a situation such as having a child with schizophrenia, it can be easy to fall into the error of claiming rights over the patient that one does not have.
A brother even told me that since the patient did not know what was best for him, without having notable disruptive behaviors other than changing some furniture of place, it was philosophically legitimate to force him to take neuroleptics, when the patient does not trust Western pharmacology at all and opts for the Oriental.
Another case: a patient who consumes beer and hashish, who has hardly any positive symptoms, but who enjoys the effects of these substances. It is clear that the mother's demand (that her son stop using) does not have much to do with the schizophrenia and it would not be necessary to fight to achieve that objective when the patient does not from far. In any case, the most common demand is that the user "do something."
After the evaluation from the perspective of the family member, we are asked how to produce the hitch. Let us bear in mind that profound inactivity and / or lack of adherence to medication are criteria for inclusion in the service. Put yourself in the patient's shoes for a moment. You are at home and one day they tell you that a psychologist is going to appear (they can confuse him with psychiatrist and get into the bag of "those sons of bitches" who never want to see again) to talk to you. It is shocking, even more so when there are interpretive biases of a paranoid cut.
I try to ensure that the shock is not so severe by asking the family member to express to the patient the idea that there is a person at his / her willingness to bring relief from the suffering that he has through any area (and only those) that he wishes to select for to intervene. Many times the response of the patient is that he does not need any of that. And many other times, the only thing the family member can do is tell him that a psychologist is going to see him, perhaps without telling him what day so that he does not "escape." Sometimes we have appeared without notifying you, but the result has generally not been favorable.
Then comes the moment of first contact. We come across situations such as, for example, speaking through a door with the patient, sitting on the floor. Or even make us meet in a corridor of the Association so that the family member introduces us when the patient left computer science class. And in that first moment We speak, generally, of anything before schizophrenia.
Let us bear in mind that the consciousness of illness has tended to be divided into three components: the proper shower awareness, acceptance of treatment and requalification of experiences psychotic. SAD patients may not have any of these components. So we focus on generating motivation in the search for reinforcement for the patient, as well as reiterating the relationship between activity and mood.
We have to fight against the fiercest enemy that a psychologist can have:
Resistance to treatment.
Evaluations that produce "resistance" may be the result of the perception of disability. Thoughts like "it should be easier, improve with it takes terrible efforts, it should get improve in a short time, I am completely disabled to do anything, I can not anymore, I can evade without consequences..."
Faced with these interpretations, we fight so that they reach these others:
- no one said that getting better had to be easy.
- It is not written anywhere that it has to be that way.
- It may be tough, but the efforts will not be titanic.
- Whatever happens, no matter how hard it may be, it won't be unbearable.
- and the effort that must be made to improve will not be either.
- doing nothing is choosing the most difficult path, that of going wrong.
- to avoid is to make a decision, you cannot not decide ...
- having some limitation does not mean being invalidated.
- Just because something has gone wrong does not mean that it will always turn out that way.
- If it is a stressful activity, it can always be remedied.
- nothing to lose.
But with this it is not enough to explain why there are patients who deny that that supposedly suits them so much. The concept of "resistance" has been widely criticized by posttrationalist models since they see in it, once again, the concept of the patient as incapable of knowing himself and knowing what is convenient for him. What I mean by this is that it would be necessary to look further, what meanings are put at stake for the patient. Recently, on a first visit, a user told me: "I can't assume that I have schizophrenia, I just can't... It would all fall apart! "This example clarifies the terror of massive invalidation or nuclear constructs and its consequent motivation towards the status quo.

Activity.
Unfortunately, the patients who come to us are not early cases in which the intervention could produce (according to Max Birchwood) a reduction in the probability of relapse by up to a quarter. So the marked inactivity is more ingrained. It seems increasingly demonstrated that constructs related to behaviors and emotions form a fragmented system in people with schizophrenia. They find it difficult to discriminate between different constructs as much as to integrate them hierarchically. Against that we fight when We can propose the activity based on a verbal search of the reinforcing capacity of what excites him, the one that other activities had at another time, those that he sees that they have in others or ultimately as a simple distraction strategy.
Distraction can be crucial when they are in stressful family climates (that is, ambiguous, complex, unpredictable, critical, hostile or with excessive identification between their members).
Hallucinations and delusions.
60% of the subjects with schizophrenia suffer auditory hallucinations and 29% visual ones. It is already known that beliefs about the omnipotence, identity of voices, and their purpose have been associated with decreased disturbance. A method of intervention in delusions has also been developed (incorrect inferences about external reality, incorrect not both for their falsity and for being taken in an inappropriate context, with an inappropriate and deeply disturbing justification).
The voices: the first reaction to the voices is perplexity. From a cognitivist perspective, these voices need not constitute a problem for the individual. It seems crucial to give importance not to the fact of having or not the voices but to the beliefs about them. Beliefs about the omnipotence, benevolence and malevolence of voices. All the voices, in an experiment by Chadwick and Birchwood, gave the feeling of knowing all about the past stories of the people who had them, what made them feel exposed and vulnerable.
Specifically, beliefs about malevolence could focus on the fact that they were a punishment for some bad action or a persecution that they did not deserve.
Faced with these different interpretations, certain behavioral and affective responses: o a commitment to voices and subsequent cooperation (generating positive affect), resistance to voices, and combative behavior towards them (which produced negative affect) or indifference with lack of involvement towards the voice (with affection neutral).
As at the point in the development of the group sessions in which we introduce the treatment of voices there is already established a therapeutic relationship, questions such as anticipating the voices positive consequences of therapy, the possibility of meeting other people with similar experiences or the non-obligatory nature of any of the activities have already been agreed.
Regarding therapy, at first the evidence that is considered less central about beliefs about voices, for example, the omnipotence of the voice, benevolence or slander, giving examples of small inconsistencies and irrationalities, to then offer the possibility of an alternative. Then the possibility is raised that the voices are generated by oneself, always having a remarkable personal meaning, as is the case (we'll see later) with possible thoughts intrusive.
The belief that voices cannot be controlled, that is, that one cannot (consequently) turn them on or off, is tested. After that, it is analyzed what antecedents trigger or diminish the voices. Which gives evidence, little by little, that the origin is internal. There are those who affirm, not without logic, that the interpretation of voices as something external is in itself a delusional belief. In addition, it seeks and verifies the significant relationship of the voices with the life of the subject, in the style of new therapies such as schema-centered cognitive therapy.
For the delusional ideas the process is very similar. In an environment of collaborative empiricism, avoiding labeling the subject as "a schizophrenic", the challenge phase begins verbally questioning only the evidence of the less grounded belief (as in cognitive therapy of the depression).
From the constructivist point of view, the intervention, being consistent with the hypotheses of Bannister, Feixas and Cornejo, Lorenzini and Sassarola, is aimed at achieving greater integration of the system, this is to achieve a clear hierarchy that increases capacities predictive. This would be carried out by separating the poles of homogenized constructs, this is separating the poles and making the construct effective when discriminating against other level constructs lower. In this sense, the ascending and descending scaling techniques can be very useful.
Depression.
The paranoid attributional style It is in clear opposition to the depressive, however, the negative affects and specifically the depressive are remarkably generalized in people with schizophrenia. It is associated with three issues: the perceived impotence of the individual who believes that he has lost control over his mind, self-evaluations negative (such as being responsible for symptoms or not being able to achieve certain aspirations makes them unworthy or lose value as people) and, finally (but, from my point of view, as an expression of the previous ones) the malevolence of the voices, which we already saw in the previous point.
Group intervention for depression includes a fictionalized story (there is a clear need for transmitting information to this population is necessary to be simple, repetitive and emotional) with two characters. One of them with poor coping and the other with useful coping.
It is about, through cognitive debate more basic, the three columns, and an arsenal of useful beliefs, to get to raise the tolerance to frustration, in the perception of themselves as absolutely useless and of the future as black.
His self-concept does not escape the ravages of having schizophrenia. The application of constructs that are not coherent with those of their own repertoire on themselves produces, thanks many times to the social stigma that accompanies them, a notable guilt.

Anxiety.
People with psychosis often report that feelings of acute anxiety, despair, loneliness, worthlessness, and rejection they are as important or more than the properly psychotic symptoms. Multiple studies have shown the importance of the perception of threat to the construct system that is revealed in anxiety. It is not difficult to imagine the number and variety of threats that can appear in the life of someone with schizophrenia.
Both those related to hallucinations or delusional ideation and those related to the threat to self-esteem or "well-being". In the anxiety section we have selected the threats and management strategies related to the latter. As in obsessive-compulsive disorder and, more broadly, in personal construct therapy, the techniques of "exposure" are understood as experiments in which to validate or invalidate the dysfunctional construction anxious. Understanding behavioral techniques in this way, they can be easily integrated into the theoretical framework that this text surrounds.
We do not always understand anxiety as an emotion "to control" or "to diminish". The re-labeling techniqueOn, for example, is a sample of how a functional meaning can be attributed to sympathetic activation, while breaking the linear model of understanding emotion as a succession (and only a succession) of cognitions "irrational".
We treat anxiety with the following techniques:
- definition
- capturing and modifying with the three columns of thoughts technique that there is a threat to my comfort, I have to
- get what I want, if I don't get it it will be a disaster.
- There is some threat to my self-esteem, I have to do things to be approved by others, I need their approval, if I don't get it, it will be terrible.
- use of rational-emotional imagination, which is difficult for them.
- activation control through Mattick's breathing adapted by Professor Echeburúa.
- use of self-instructions.
- relabeling of anxiety.
- positive practice.
- on a separate sheet, EMDR and income.
Aggressiveness.
Regarding aggressiveness, we have tried to make the relationship between aggressive "behavior" and the user's personal meaning. The dominant narrative in which the value of people is understood as dependent on successes, failures, praise, insults, achievements, merits, etc. entails the need to reinstate the "lost" value (often tacitly, only translatable into words with verbs of the type "carries", "implies", "is inexorable..."). The influence of values determined by economic-social factors is evident ...
- Definition and origin in oneself, not in others, attacks the one who can because most of the time it is associated with undervaluation and an attempt is made to prevent... Given the opinion that in the face of certain attacks it is impossible not to respond, it is refuted by treating it as an algorithm. Why should answering like this be inexorable?
- discuss absolutist thoughts in the second person.
- debate thoughts of injustice.
- discuss thought reading.
- analyze advantages and disadvantages.
- find part of reason, the non-aggressive intention of the other person, draw norms and when you used that norm yourself.
- "turn blue", get out of the situation before reaching the red.
- positive practice
Obsessions and compulsions.
In this issue cognitive therapy has made remarkable strides in recent years Once again, it is not the event that brings the unpleasant consequences. Interpretation presents itself again as the key; with a peculiarity, the antecedent is not an external event, but ideas, images or impulses that only the user knows. Metacognition about these events is the central axis of intervention techniques, both in the interpretation of increased occurrence of an event (fusion-thought-action), as in the relationship with the user's ethical principles (thought-action fusion of the moral). In this way, the application of constructs of the self that are not congruent with those of the person produces, as a result of the obsession, guilt.
We have also found in this case another reason for replace the concept of "self-control" with self-management. Control becomes your worst enemy here.
- Following the intervention program of the Jaume I University of Castellón, by professors Cristina Bottle, Rafa Ballester and Miryam Gallardo, we give the definition and origin of intrusive thoughts and their contents. We exemplify with a list of intrusive impulses and thoughts from Rachman and Silva.
- We question metacognition, following the guidelines of Wells, (1997) with which we analyze what happens if a person interprets that thought as valid or not.
- We apply a list of questions to challenge metacognition, such as "to what extent would you feel responsible if you think that thought has no value? To what extent does checking help you to solve the problem?"
- We give instructions regarding thought-action fusion, trying to break the association between the occurrence of having a thought or impulse and the probability that it will happen. In one case of SAD, I asked the patient to imagine that he murdered me on the spot and to tell me about it. Then I imagined that I was murdering him. He was very surprised to find that I did not blame myself for having thought about it and that neither of them had murdered the other.
- We give instructions for self-exposure, its logical basis and exposure to one's own obsessions and what is feared. Bearing in mind that the goal is to check live to modify beliefs.
- We try to arrive at a new phenomenological attitude with acceptance of thoughts, of the flow of consciousness, suspending any type of judgment on thoughts. This single recommendation served to reduce suicidal ideas and impulses (apparently depressive) in a few weeks until almost disappearance in the patient mentioned above.
Family intervention.
From the cognitive and systemic perspectives, the interpretation of the behaviors of others and their repercussion on oneself are of crucial importance.
It seems clear to us that, when several people interact for a certain time, a system emerges of constructs, of characteristics applied to others and to oneself, as an entity by right own self. Each individual can have a unique position in the construct system but these positions depend on each other in a dynamic equilibrium.
On one occasion, a patient told me about his vision of his rightful place in the family: "I think my sister is confusing her roles. Being a psychologist is no reason for her to tell me what to do... or for her to try to become my friend by being my sister. And my father... my father comes home after fighting, the day is a battle, society is like that; if he left the armor at the door... But it doesn't. So, of course, ha! Yeah, yeah, yeah... They say that when they talk to me I lose the ball. But, how can I not go if it is the only way I have not to argue ???"
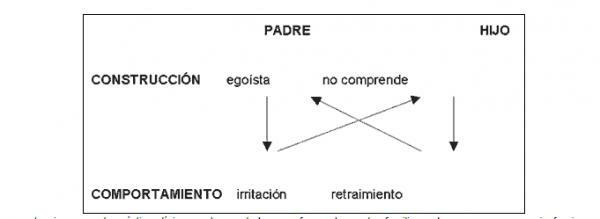
The formulations that we make can be represented as follows: A father may be angry with his son because he seems to be wringing the bag with respect to the family. The son withdraws and becomes mute, since the father's irritation "shows" that he does not understand him and will never understand him:
There are some evaluations that clinical practice has revealed to us as frequent in the relatives of people with schizophrenia, and that, as you all know, can raise the level of perceived stress reflected in the expressed emotion. Max Birchwood has found that the attributions of relatives towards the patient's control of his own symptoms are indicative of a greater behavioral disturbance of the patient. Thus, a first group of dysfunctional evaluations are similar to "he could get out of this if he wanted to, just by trying." His behavior is caused by his laziness or his irresponsibility. "
Secondly, absolutist thoughts according to those attributions: "he has to stop doing that, he has to behave according to family rules."
As a complement, evaluations that do not consider context appropriately and they exaggerate the consequences: "it is terrible that he does not comply with that norm, I cannot bear to see him lying down", which reflects an extreme rigidity to new experiences and an intensional perspective, in which language moves away from the facts and leads to interpretations of the type "everything does it its own way. way".
The intervention, after evaluating the evaluations of each member and their communication style, seeks a new construction of meaning in each member of the family about the behaviors of others and about themselves themselves.
A few notes regarding substance use.
There are three reasons that lead a person to use the substance:
- self-medicate bothersome symptoms,
- get the external approval
- or by hedonism, which may seem quite logical given their inability to enjoy under normal conditions.
Each cause will have a different strategy: improve the medication they take, teach assertiveness skills after modification of the assessment in which they believe they "need" external approval and a search for alternative activities pleasurable. It is true that there are cases in which the use of substances is perfectly reasoned, and there are few arguments left to find the discrepancy between their objectives and the use of the substance. For example, a case where hashish was the only way to facilitate gratifying visual hallucinations
Therapy for therapists.
To finish, and since for being therapists we do not stop being human, I show you some evaluations of a co-therapist:
- I'm never going to be a good therapist.
- I can't get hooked on patients.
- Alejandro is thinking that I will never work as a psychologist.
- I've been late again, I'll never be formal.
- I'm sure he disliked me, he is horrible.
This article is merely informative, in Psychology-Online we do not have the power to make a diagnosis or recommend a treatment. We invite you to go to a psychologist to treat your particular case.
If you want to read more articles similar to Cognitive Therapy in a Home Care Service, we recommend that you enter our category of Cognitive psychology.
Bibliography
- Aldaz, J.A. and Vázquez, C. (comps.) (1996) Schizophrenia: psychological and psychiatric foundations of rehabilitation. Madrid: XXI century.
- Bannister, D. And Fransella, F. (1966) A grid test of schizofrenic thought disorder. British Journal of Social and Clinical Psychology, 5, pp. 95-102.
- Bannister, D. And Fransella, F. (1967) Grid test of tought disorder. Barnstaple, England: Psychological Test Publications.
- Beck, A.T. (1976) Cognitive therapy and the emotional disorders. New York: International Universities Press.
- Beck, A.T. (1997) Cognitive therapy: past, present and future. In Mahoney, M.J. (ed.) Cognitivist and constructivist psychotherapies: theory, research and practice. Bilbao: DDB.
- Beck, A.T., Rush, J., Shaw, B. and Emerg, G. (1983) Cognitive therapy of depression. Bilibao: DDB.
- Bello, A. (2000) Cognitive Therapy in a Home Care Service. Presentation at the II Seminar on Advances in the Evaluation and Treatment of Schizophrenia. Spanish Association of Behavioral Psychology. Grenade.
- Bello, A. (2001) Anorexia and Capitalism. Article in http://www.nodo50.org/caum.
- Bello, A. (2002) Programs of Attention to Families. Presentation at Conference on Mental Health and Chronicity. Madrid: IMSERSO.
- Bello, A. and Crego, A. (2001) Globalization and Mental Health. Article in http://www.nodo50.org/caum
- Birchwood, M. And Tarrier, N. (1994) The psychological management of schizophrenia. Chychoster: Willey
- Billing, M. (1987) Arguing and Thinking: a Rhetorical Approach to Social Psychology. Cambridge: Cambridge University Press.
- Bottle, C. (1999) Obsessive-compulsive disorder. Madrid: UNED- Fundación Universidad Empresa.
- Bottle, L. (1993). Emotions and construction of meaning: Therapeutic implications of the constructivist conception of emotional processes. Revista de Psicoterapia, 16, 39-55.
- Bottle, L. (1996). Different paths to the same goal: The construction of constructivism in psychotherapy. Journal of Constructivist Psychology, 9, 233-247.
- Bottle, L. (1998a). Clinical psychology, psychotherapy, and mental health: Contemporary issues and future dilemmas. International Journal of Psychotherapy, 3, 255-263.
- Bottle, L. (1999). Constructivism and constructionism in family therapy: Pragmatics, semantics and rhetoric. Argentine Journal of Psychological Clinic, VIII (2), 121-133.
- Bottle, L., & Gallifa, J. (1995). A constructivist approach to the development of personal epistemic assumptions and worldviews. Journal of Constructivist Ps
- Bottle, L. (1997a). PCP in a changing Europe: From the matrix of decission to multiphrenic identity. In P.M. Denicolo & M.L. Pope (Eds.). Sharing understanding and.


