Mom: I don't want to go to school, my head hurts a lot, my tummy hurts a lot!
Mom: I want to sleep with you, I'm scared! Do not turn off the light! Do not leave me alone...
Mom: I'm not scared to the yayos' house! Do not go! Help a dog, a spider... I can not drive! I can not eat! I can't get in the elevator! I can't go to the theater! I can not leave home!…
Fears are normal experiences in children's lives. Given the need to shed light on this issue, at PsicologíaOnline, we offer this article on Fears, Anxiety and Phobias: differences, normality or pathology ?.
Index
- Fear as an emotional response
- Anxiety as a psychophysiological response
- Phobias as an uncontrolled and disabling response
- Different hypotheses about the origin of fears
- Most common fears in childhood
- Most common fears in childhood II
- Specific phobias
- Social phobias
- Agoraphobia
- Therapies
- recommendations
- Attitudes that can prevent the appearance of phobias
- 10 rules for dealing with panic
- Final reflection
Fear as an emotional response.
Fear is a normal and universal emotion, necessary and adaptive that we all experience when we are faced with certain stimuli both real and imagined, children throughout their development will suffer and experience numerous fears: separation, strangers, loud noises, darkness, being alone, animals, school and so we could continue with a very long etc. Most will be passengers and will not represent any problem, will appear and disappear depending on age and psycho-neurological development.
These fears, through learning, will be very useful on many occasions as they can help them to cope adequately and adaptively with difficult, complicated, dangerous or threatening situations that may arise throughout their lives and its fundamental function will be to protect them from possible harm generating emotions that will be part of their continuous evolution and development (the child should not be afraid of slides, for example, but should be cautious when going down and playing on them).
Therefore, it will not only be normal but also necessary for children to experience specific and concrete fears. in situations, objects and thoughts that imply danger or real threat, thus avoiding running potential unnecessary risks that could endanger your life, health or physical well-being or psychological, but without these being at any time important enough to significantly alter your life or your cognitive or emotional development.
Anxiety as a psychophysiological response.
Anxiety is a psychophysiological alarm response that arises when the person needs to react to certain situations, stressful events or stimuli perceived as threatening, dangerous or uncertain, whether real or imaginary, internal or external. Like fear, it is also a normal, necessary, adaptive and even positive response. as it prepares the body to mobilize in situations that require neuronal activation greater than that required by many other situations that do not imply any difficulty.
While the state of alarm or alert lasts, the body sets in motion a series of defense mechanisms, both physiological and psychological, in order to overcome and face the possible threat and although during this time the feelings, not pleasant, of anguish and insecurity increase also greater perception of the environment and greater mental acuity and concentration are increased in addition to a better physical preparation to facilitate that the confrontation with the threat can be carried out with the greatest possible success and we can even increase our performance as long as the anxiety response ends as soon as the triggering anxiety factor ends.
Fears considered normal and dependent on maturational development:
0 to 1 year
Fear of strange or violent stimuli, loss of support, strangers, separation from parents... (They are considered genetically programmed and of high adaptive value as they will help us survive against possible threats or dangers)
2 to 4 years
The evolution of authentic childhood fears beginsMost fears of animals begin to develop at this stage and can last into adulthood. We find ourselves in fear of falls, animals, strangers, loud noises, darkness, cars, separation from parents, changes in the environment, to the masks... (the child can explore his environment so the fears are increasing since there is a greater probability of encountering situations of danger, avoidance responses appear fleeing the frightening stimulus and running to meet the parents) (the nature of fears and cognitive development also changes because of what fears take on a more social character and usually they gradually disappear as the child grows up and faces them)
4 to 6 years
The fears of the previous stage remain but the stimuli that may potentially be capable of generating fear are increasing such as, loud or strange noises (sometimes the product of your imagination), thunder and lightning, bad people, changes in the environment, masks, heights, catastrophes, and imaginary beings (monsters and ghosts), bodily injuries, sleeping alone or staying alone... The cognitive development of the child and his fantasy capacity are at these older ages For this reason, imaginary stimuli enter the scene, the most varied situations and diverse phobic stimuli are added that can last until adulthood.
6 to 9 years
The child achieves the ability to discriminate internal representations of cognitive reality. Fears will now have greater realism and will be more specific, little by little the fantastic world and the fear of imaginary beings will disappear but more specific and concrete fears will become more relevant such as fear of the dark, physical harm and injury, criticism or ridicule for the lack of school and sports skills, school, school failure, animals, to be observed, to physical appearance, the fears transmitted by the media also increase. communication… Little by little they will disappear some fears and others increasing depending on how they got through the small confrontations that have been presented throughout its short life.
9 to 12 years
As in the previous stage cognitive reality is gaining more relevance, they begin to become aware of concrete and specific fears but more based on objective reality such as fear of fire, thunder and lightning, exams, academic achievement, school failure, bodily injury, accidents, contracting serious diseases, death, the sense of ridicule increases, the fear of serious conflicts between parents (fights, separations, divorces) or poor school performance, the fear of classmates increases and especially those who show themselves aggressive. At these ages there is usually a slight rebound in fears that seemed to be overcome.
12 to 18 years
In this stage fears of animals and specific stimuli are reduced to go giving step to fears related to personal self-esteem (intellectual capacity, physical appearance, fear of personal or school failure) and social relationships (concern about rejection or recognition by peers, classmates ...), criticism... In this stage family distancing begins and the need to experience new risks As a way of asserting themselves within the group of friends, little by little they will leave behind the childhood stages and the group they belong to will take center stage.
From 18 years old
Fears will evolve due to learning, to own experiences or witnessed in other people's, some will be necessary and adaptive They will help us to be in a state of alert and caution in the face of the different situations that may require it and we will come out stronger, others will overcome without leaving any trace but others will lead to real phobias with all the consequences that may arise from it. Hence it is It is essential to prevent, solve and acquire the necessary resources and skills to be able to face and respond satisfactorily to the environment both internal and external and prevent a fear that in principle is adaptive from ending up leading to a phobia that is no longer adaptive but pathological.

Phobias as an uncontrolled and disabling response.
Fear and anxiety are no longer normal, adaptive, necessary and positive responses when exceed the tolerance threshold, there is no perception of control, there is a continuous avoidance of the aversive stimulus, they interfere considerably in the normal and adaptive functioning.
The answers continue to be maintained despite the amount of rational explanations they may receive in this regard, since terror disables them to listen to reasons or make rational decisions before real or imaginary situations or before objects and animals that for most people do not pose no danger except to whom your brain interprets them as terribly dangerous and threatening. These responses are excessive and they come loaded with a considerable, continuous and persistent state of anxiety, They are unreasonable and intensely disproportionate, are prolonged in time Y generate clinically significant discomfort with enormous suffering, suffered by both the child and the parents or adults who care for him, presenting a set of symptoms that they can become incapacitating for the person who suffers them, generating all this a state that escapes the mechanisms of control.
In this situation the fear turns into a phobia, where there is no longer fear but panic, and anxiety stops being positive to become negative and pathological which makes it highly damaging and damaging to those who suffer from it, as well as significantly altering their ability to cope with situations everyday life (such as sleeping, being alone or with people, going to school, leaving home, traveling, facing different situations that will depend on the object feared, etc. and ultimately to be able to lead a normal and satisfying life).
Drawing the line between fear, anxiety and phobia will not always be easy It will depend on factors such as age, nature of the object or feared situation, frequency, intensity, degree of disability, etc.
Faced with a phobia, the most disparate behaviors will occur and with great difficulty to maintain a rational control of thought, reacting from absolute immobility to panic attack where the norm is great avoidance of aversive stimulus or with a desperate and uncontrolled flight when it cannot be avoided and there is no choice but to be exposed to it.
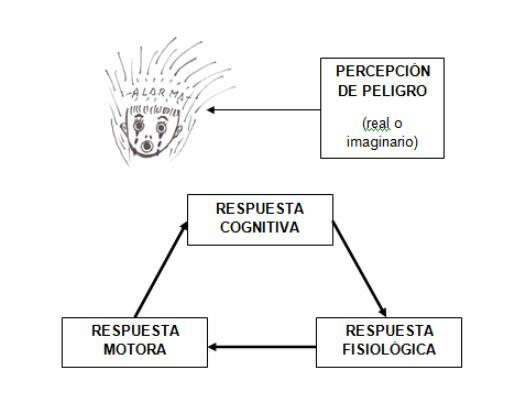
To better understand what happens to a phobia, we can analyze the manifestations through three levels of response: the physiological, motor and cognitive.
Cognitive response
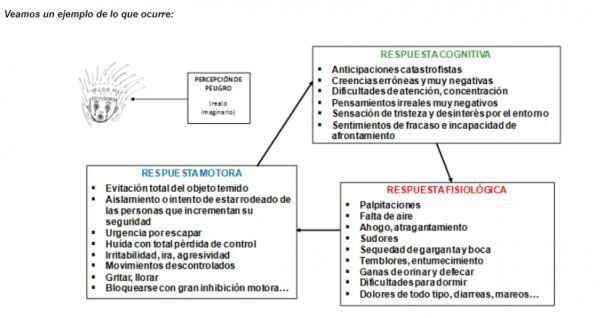
Refers to all thoughts, beliefs and images all with a great content of danger or threat and derived from the perceived fear of the phobic stimulus. These thoughts occur automatically with total perception of loss of control, great conviction that it will not be able to be borne, that the worst will always occur with great anticipation of all kinds of disasters... The anticipation will be totally negative and even long in advance. In general we will find:
- Large number of subjective anticipations related to physiological reactions
- Large number of erroneous, negative and irrational beliefs regarding the feared situation
- Great physical and mental fatigue
- Difficulties with attention, memorization and mental concentration
- Altered space-time perception
- Unrealistic, distorted, very negative and catastrophic thoughts
- Feeling of unreality, sadness and great disinterest in the environment
- Feelings of failure and inability to cope
- Fear of dying, suffocating, having a heart attack, having an accident, losing control ...
Physiological response
Includes all internal demonstrations that we can feel when we are faced with the phobic stimulus, the sensations will vary from some people to others depending on the type of phobia, which for some will be fundamental for others may be irrelevant. A person who is afraid of having a heart attack will fear palpitations, tachycardia, pain in the chest or arm... while a person who is afraid to eat in places that do not controls, due to what may happen to him, he will not bear minor abdominal discomfort, choking sensation, nausea... Among the most common physiological manifestations we can find the following:
- Rapid heart rate, palpitations
- Severe chest tightness, chest pain or discomfort
- Feeling of shortness of breath, choking, choking
- Excessive sweating
- Throat and mouth dryness
- Urge to urinate and defecate
- Tremors, paresthesia (numbness of limbs or tingling sensations)
- Sleeping difficulties
- Muscle, headache, abdominal pain ...
- Gastric acidity
- Digestive disturbances (diarrhea or constipation, nausea, vomiting)
- Feeling dizzy, vertigo and even loss of consciousness ...
Motor response
Includes all those behaviors aimed at avoiding, running away, seeking help and safety, isolation, doing anything that allows them to escape or escape danger... Some will go to the emergency room at the slightest physiological manifestation, others will not leave home without taking anxiolytics or drugs with them. drugs that give them the necessary safety, others will avoid activities that involve physical effort, others will not eat certain meals, others will be unable to be left alone, to speak in public, to socialize, to ride in a car or any other means of transport... Each one will avoid everything that is to a greater or lesser extent related to their phobia. In general, we will find:
- Total avoidance of the feared object
- Isolation or attempt to be surrounded by people who increase security
- Urgency to escape, flight with total loss of control
- Irritability, anger, aggressiveness, uncontrolled movements
- Screaming, crying, blocking with great motor inhibition ...
These three responses, cognitive, physiological and motor, will always be present and closely interrelated when an abnormal state of anxiety is activated.. Therefore, as soon as we modify any of them, we will automatically modify the other two, so it will be vital It is important to know them thoroughly to be able to expose ourselves and face the vicious circle in which the person who suffers remains hooked. a phobia.
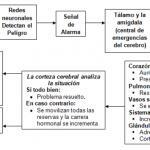
In addition to the comments, we will also encounter biochemical changes as increased secretion of adrenaline, norepinephrine, fatty acids, corticosteroids... and ultimately with a nervous system willing to generate everything that is necessary to face the needs of confrontation, fight, flight or, where appropriate, return to normal. Due to sensory impulses (coming, for example, from the eyes) neural networksthey detect the danger, are activated and give the signal from "Alarm" which is first transmitted to the thalamus. If he thalamus and amygdala (emergency center of the brain) consider the stimulus as dangerous, automatically launch the general alarm and fear, anger or any other emotion comes out on the scene and spreads in tenths of a second throughout the body through thebrainstem what causes different physiological changes in the organism that they prepare you to face danger, whether real or imagined.
- The heart and breathing accelerate, increases heart rate and blood pressure. By getting the muscles to receive more blood, they can eliminate more toxins and the flight or defense is facilitated as well as greater oxygenation.
- Cutaneous blood vessels narrow so that less blood flows through them and benefits especially the internal organs.
- The immune system mobilizes additional battalions of defensive cells to face the consequences caused by the threatening situation.
- The adrenal glandsactivate the release of adrenaline which ensures that the brain and muscles have an additional supply of energy.
The body is ready for flee or defend. One time passed thisfirst reaction phase the sign of "Danger" arrives to the cerebral cortex where he resides conscious thought Y that's where the situation is really analyzed. If the brain through thought also qualify the sign as "danger" (for example, a threatening situation for us) the reaction intensifies. And it is from this moment when the hormonal race begins through the brain and throughout the body. The goal is once again in the Kidney glands what now they will secrete cortisol. This hormone further sharpens the body's reaction Y will be in charge, among other things, of maintaining the answer mobilizing sufficient reserves so that the energy supply is adequate. Later, once the perception of danger has passed, it will be cortisol itself that takes care to give the stop sign and that the system returns to its normal situation, putting an end to the situation.
The function of all these changes will be to keep us safe when we are faced with a real danger because in addition to mobilizing to avoid it, flee or seek help It will also make us learn to avoid similar situations in the future that really represent a danger. The problem will arise when the alarm reaction is triggered uncontrollably and without a real danger sustaining it. In this case it will be the person himself who starts the whole system alarm interpreting the situation as dangerous based on sensations that he experiences or perceives as such by the mere fact of thinking that he is facing a danger regardless of whether it is real or imaginary.

Different hypotheses about the origin of fears.
As we see fears are very common and in principle Although almost all children experience anxiety and fear at some point in their life, these fears are normalappear for no apparent reason, are subject to an evolutionary cycle and tend to disappear over time as the cognitive, social, maturational or emotional characteristics, except for the fear of strangers that can persist during adult life giving with greater intensity in cities than in towns, where almost everyone knows each other and the perception of danger from strangers is less intensity. We will only worry when they interfere with daily life. and it must be an expert who determines if it is about fears inherent to evolutionary development or on the contrary it is a problem that must be solved to avoid future problems.
Through numerous investigations it has been revealed that girls tend to present more fears and of greater intensity than boys.
There are various hypotheses in this regard as the biological according to males would be better equipped for attack and defense showing less fearful behaviors by being constitutionally stronger.
The sociocultural whose explanation would be given by the differences determined by the social roles transmitted to each sex depending on the social environment in which it develops. Girls are more permissive when it comes to expressing feelings and emotions related to fearful situations. Girls are not required to be brave or face risky situations with the same intensity as boys. child, they are shown affection and understanding when she feels fear, the child on the contrary is required to be the strong, the launched, the one who faces and the more courageous the greater reinforcement receives both from parents and the environment, this differentiating attitude will gradually shape and modulate their behaviors of exposure and confrontation with the afraid.
However, each one depending on their personal characteristics or their own experiences will develop or not different fears that can lead to phobias. but regardless of genetic programming to develop normal evolutionary fears that play a clear factor of survival, of individual differences or of sex, we also find multiple factors that can influence the development of phobias such as familiar patterns this hypothesis would explain the phobias based on behaviors learned by observing models "Learning by modeling" (especially through parents or close friends). Fearful parents may be unintentionally, through their behavior and emotions, inducers of establishing different fears in their children “Fearful parents will transmit insecurity to their children and fears ”.
At other times it will be a consequence of the direct or indirect experience, a child or an adult who has been bitten by a dog, or has seen how a dog has bitten another person, is very likely to experience Phobia of dogs and even spread to other animals by generalization, at other times uncontrolled fears will come determined for verbal instructions coming from the environment as a way to control behavior (The coconut is coming, the bogeyman will come and take you away, if you behave badly, the pirula witch will come and take you to her cave ...) or by the media or through movies that are presented as threatening or terrifying and even the cartoons themselves will be the cause of generating different phobias in children. At other times, in our spirit of providing protection, we will overprotecting and preventing them from facing by themselves normal or complicated situations that allow them to develop their intellectual curiosity, resources and skills to cope with them or promote independent behaviors and responsible.
Other times it will be unpleasant or traumatic life experiences after witnessing mistreatment, fights, serious accidents, deaths of a loved one... which impacts them emotionally, leading to more or less important clinical pictures.
At other times they will be fruit of imagination or misinformation In the face of certain physical illnesses, other many times we will be the adults themselves who will use fear to protect the children in the face of potential real and dangerous situations (electrical outlets, traffic, animals, going alone on the street, contacting unknown ...) ...
In summary we see that the origin can be diverse and the causes multifactorial, It will depend on how we act about it, how we anticipate them or face the feared objects, how let us resolve, that we do it more or less urgently, that we acquire a greater or lesser number of resources and skills of confrontation... that everything comes to nothing and disappears without leaving any sequel and we can even leave strengthened of this or, on the contrary, it becomes a true clinical picture with greater or lesser complication pathological.
Most common fears in childhood.
Fear of separation
It is one of the first fears to appear. It is characterized by an intense fear of being separated from parents, relatives or people emotionally linked to them, it is about a highly adaptive fear with great survival value, in fact its presence indicates a certain degree of maturity in the boy. Virtually all children suffer from it when they are young. Its resolution will not represent any problem and will generally do so without leaving any trace. When it comes to solving the problem, parents will play an important role as parents who express great anxiety about the separation of their children will end up infecting them. Hence, the type of parenting is essential for children to pass this stage without suffering further damage and can move towards greater autonomy.
Newborns show crying or altered behavior when they are hungry, tired or uncomfortable without this implying fear itself because they it is simply a wake-up call in search of protection and therefore a highly adaptive reaction as it helps them to survive against possible threats. It is at 6 months when babies begin to express through crying and screaming the anxiety generated by the separation from their parents or the people who care for them, fear will be more specific when children start to walk and they will manifest it by running towards their parents as soon as they perceive estrangement from the people who protect and care for them.
The child suffering from this disorder feels great discomfort when he is or thinks that he may find himself alone in the face of any type of threat. The anxiety can become so great that the child refuses to sleep alone, to stay alone, to go to school... arriving even to present nightmares related to the separation or physical symptoms such as headache, belly pain, stomach…
The normal thing is that it solves without problems as the child grows but if it is not resolved satisfactorily, its early detection will be essential, which will be determined by the degree of manifested anxiety, since it has been possible to verify its close relationship with school phobia in children and with agoraphobia in Adults.
Fear of strangers
It is an innate and universal fear. Its appearance occurs between the first and second year of age and is the most feared stimulus between six months and two years.
Before a stranger, the child will respond by looking away from her, breaking into tears or screaming and the answer will depend so much on the situation (that the child is alone or accompanied by parents or caregivers, that the situation is more or less known ...) as well as the behavior of the stranger (who approaches slowly or unexpectedly, whether or not there is physical contact ...) or the physical characteristics of the stranger (women cause less fear than men and children less than grown ups). Previous experience with strangers will also play an important role, it will be easier and will represent less fear for those children accustomed to interacting with different people than those whose relationship is more limited to the family.
It will tend to subside as we mature both cognitively and emotionally.
Fear of the dark
It usually appears around the age of two and generally disappears by the age of nine.. It can produce great anxiety at night and especially at bedtime, causing great discomfort and fear of sleeping alone or staying at dark, is generally associated with different types of fears such as monsters, witches, thieves, hidden imaginary beings that can appear in any moment…
The fear of the dark sometimes it will be accompanied by sleep disturbances such as nightmares or night terrors. Both will occur during sleep but have very different characteristics, nightmares usually appear between the ages of 3 and 6are characterized by presenting content loaded with great anxiety that they will remember clearly when they wake up after the dream, however In the case of night terrors, the awakening will be abrupt, accompanied by screaming, crying, open eyes and a great manifestation of confusion and disorientation, without the child responding to the parents' efforts to wake him up and without remembering anything about what happened upon waking after completion the dream, usually occurs between four and twelve years of age and it represents a great alarm for parents who see how the child presents these manifestations without them being able to do anything to help him. Unlike nightmares, the child will not remember anything.
School fears
School is the place where children spend most of their time and where they experience a large number of both positive and negative experiences. Fortunately it affects a minority of children and tends to occur between 3-4 years or 11-13 years although it can also occur outside of compulsory studies. Its onset in children is usually sudden, while in adolescents it appears more gradually, with greater intensity and with a worse prognosis. School phobia is preceded or accompanied by physiological symptoms of anxiety (tachycardia, sleep disorders, loss of appetite, nausea, vomiting, diarrhea, headache or stomach pain, great discomfort ...) and with great cognitive anticipation of highly negative consequences associated with everything related to school as well as great dependence on the mother or caregivers. All this will increase avoidance, disability, inhibition and blocking behaviors towards school tasks with all kinds of anticipatory anxiety behaviors. Unlike what happens with other fears, school phobia has been shown to increase with ageHence, if school failure is not fought in time it will be guaranteed, in addition to increasing many other associated fears such as fear of the teacher, of school failure, of making a fool of themselves, of reading aloud, of making mistakes, of being laughed at, of colleagues, social relationships... which will considerably reduce their safety and self-esteem with the risks that all this carries.
Among the most typical answers that we can find would be, among others, the following:
- They refuse to attend school, making up a thousand excuses and delaying their departure as long as they can.
- They cry, scream and kick when it is time to go to school and if they go to school they cry and hold on to their mother tightly so that she does not leave them.
- They complain of all kinds of headaches, stomach pain, leg pain... with a wide variety of physiological symptoms such as tremors, stiff legs or arms, excessive sweating in the hands, nausea, vomiting, diarrhea... when it is time to go to school but disappear if they are allowed to stay in home. During the weekend or on vacation nothing hurts them, they are happy and are doing great.
- They anticipate all kinds of negative consequences, which predisposes them to give highly unfavorable answers, which considerably increases their fear when their suspicions are confirmed.
- They carry out a very negative self-evaluation of their abilities, which greatly hinders their learning.
- They plan all kinds of escape and avoidance responses ...
The phobic response, in this case, is maintained and persists due to the benefit obtained by avoiding the phobic object, which in this case will be the school with everything that accompanies it: reduction of homework, more attention received, realization of much more pleasant substitute activities, with the excuse of not feeling well they can stay at home playing, watching the TV…
In the face of these fears, it will be essential to act as soon as possible, before it can lead to a phobia, to provide them with sufficient resources and skills to allow them to face different situations anxiety that will appear throughout the school process and thus avoid or hinder the appearance of future emotional disorders, school failures, social or personal.
Most common fears in childhood II.
Fear of dogs, cats, or other animals
In this case, the animals will be the cause of the fear or possible phobia and as causes of the fears we will find dogs, cats, snakes, spiders, rats and mice, flying insects and birds as the most frequent, reaching the maximum point of anxiety when the animals are in motion. In some cases it will be acquired through direct experience but in many other cases it will be transmitted through the different models who have experienced phobic anxiety before certain animals. Curiously, many do not believe that the animal will harm them, because on some occasions they have never seen them, but they are convinced that they will be terrified, that they will lose control, that they will suffer some mishap while trying to escape or have a cardiac arrest, or they will not bear the feeling of disgust or disgust that their presence may cause them or else they will anticipate so many disasters that they will avoid by all means approaching them both in real and imaginary.
Fear of animals will occur especially in childhood and will generally be transitory, but there will be occasions in which it leads to a true phobia and translates into a significant deterioration of activities everyday (resistance to going outside for fear of meeting a dog, a cat or fear of carrying out certain activities where the feared animal may cross ...) function of the feared animal, since for example it is more difficult to come across a snake than with a dog or a spider, the person will experience greater or lesser inability to lead a normal life, and this will be decisive to take the appropriate measures when deciding whether or not to go to a professional to help us overcome the phobia.
Fear of illness and physical harm
It is a universal and highly adaptive fear as it represents a real threat to the safety and survival of human beings..
Fear of injury and blood occurs in almost all children although it will prevail to a greater or lesser extent based on previous experiences lived by themselves or transmitted by family members who present a phobia both to blood and physical damage as well as to real diseases or imaginary. Accompanying the phobia can be symptoms such as breathing difficulties, rapid heartbeat, dizziness and even fainting... Fears of doctors, dentists (quite common, especially in men, there is great hypersensitivity to the choking reflex when objects are introduced into the mouth or the throat. In severe cases, choking occurs just by hearing, smelling, or thinking about the dentist or by related stimuli such as brushing teeth, fastening the neck of the shirt, wearing high or closed collars around the throat, being touched in the mouth or on the lips ...), fears of hospitals are also widespread and injections, so the attitude towards it will be decisive when establishing or not the specific or generalized phobia, preventing on many occasions that preventive controls are carried out and even the administration of treatments to certain diseases that if caught in time would not cover any trouble.
Other types of frequent fears
In addition to those seen there are many more stimuli that can be triggers of fears and that later can lead to phobias.
Among the most frequent we find:
- Fears derived from natural environments as are fears of storms (thunder and lightning), wind, water, loud noises, mountains, the sea ...
- Fears derived from specific situations such as public transport, bridges, heights, tunnels, elevators, flying by plane or traveling by boat, cars (driving or traveling) closed or open spaces ...
- Other types may refer to situations that can cause choking, vomiting, diarrhea, incontinence, contracting diseases, falling if we are not near walls or nearby means of restraint, to suffer vertigo, to speak in public, to suffer accidents, to be injured, to be caught in a traffic jam or in small places, to physical sensations, to lose control, to pass out, to go crazy, to have to defecate or urinate outside home...
It has been proven that in general having a phobia of any kind increases the possibility of having fears (not necessarily phobic) of one or more of the other fears. In addition not all phobias share the same clinical characteristics the differences will depend on age, the onset of the problem, sex, the pattern of physiological, cognitive or motor response, subjective experience and objective, situation, family history, interference in daily routine, time spent planning what to do to avoid the object phobic, etc ...
Most phobias are considered to derive from specific basic fears hence the importance of preventing and resolving them before they become clinically fears significant because unresolved fears can lead to future phobias in both children and Adults. It was previously thought that phobic fears in childhood and adolescence could remit without psychotherapeutic treatment but the evidence shows that the general trend does not seem to be this and in general We can say that the greater the number of specific phobias or specific fears accompanying them, the lower the probability of recovery..
Specific phobias, also called simple or focal, represent a small part of the phobic disorders seen in the clinic and this may be because most patients do not seek help and when they do it is because They already have very high levels of pathology which considerably disables them to develop a normal life, among the most frequent consultations we find with:
Specific phobias.
They are very common in both children and adults. In both cases they can be overcome without major difficulties with psychotherapeutic treatments. Phobic stimuli will be concrete and specific situations or objects such as animals, darkness, water, heights, elevators, driving, traveling by plane or other means of transportation, closed or open places, injections, eating specific foods, dentists, contagion of diseases, defecation or urination in public places, firecrackers and fireworks... Specific phobias usually appear during childhood or adolescence, have a tendency to persist into adulthood and if not treated in time they can persist for decades. The degree of disability will depend on how easy it is for the person suffering from it to avoid the phobic situation. People who suffer from this type of phobias are aware that their fear is irrational and disproportionate to real situations, comes triggered by the presence or anticipation of the phobic stimulus Y they avoid it by all means at their disposal. Exposure or anticipation of the phobic stimulus will immediately cause great anxiety, they even fear the panic they may experience and the consequences negative that may derive from it, so its anticipation will be continuous as well as its avoidance, in case of not being able to avoid it, the anxiogenic manifestations will be so They are still going to be convinced to a greater degree of the need to continue avoiding it, continually finding themselves in a vicious circle from which it is impossible for them leave.
Social phobias.
Like the other phobias the social phobia is characterized by extreme fear, exaggerated, disproportionate and loaded with great anxiety in social situations that for most people will not represent any danger real but that, however, for those who suffer from it, will make it impossible to react normally to situations in which they can be observed by others, have to speak or act in public, interact with strangers, perceive that they can be evaluated or analyzed in some way way,… They are hypersensitive to criticism, with low self-esteem, with deficits in assertiveness and social skills, with exaggerated fear of feeling rejected, humiliated or criticized, they themselves are exaggeratedly self-critical, so they will avoid all those social situations or actions in public that may put them in evidence in a way or other. Often they will develop generalized anxiety disorders and depression and may even turn to addictions as an attempt to solve their social deficits.
It seems that social phobia is suffered equally by men and women, generally usually appears in adolescence with a history of shyness during childhood. It can appear as a result of an experience experienced as stressful or humiliating or slowly due to to a continuum of situations in which the person, due to their social disability, experiences them with a great burden of anxiety. The evolution is usually chronic with a tendency to worsen and persist throughout life if it is not treated effectively by psychotherapy. Generally those affected do not usually seek help, perhaps because they consider that it is something unchangeable and inherent in their character and when they do is for serious personal, work or social reasons that prevent them from carrying out activities necessary for daily performance normal.

Agoraphobia.
Being the phobia with greater disability given that it can imprison people in their own homes, it is perhaps one of the disorders most frequently seen in consultation, especially women. It is a pathology in which more and more situations are being avoided until a time comes when they can no longer even leave their own homes. The anxiety they experience just thinking that they may be trapped in some place or situation where they cannot escape or find help, in case of an anxiety or panic attack, It is so big that it leads them to take all kinds of measures and precautions that make it impossible for them to be in crowds, queue, travel by means of transport, go to theaters, supermarkets, restaurants... For them, any place can represent a problem, so they generalize to multiple situations and stimuli, due to the association that occurs between the internal sensations perceived as highly alarming and the evaluation of both real and imaginary danger that is made in this regard, in such a way that each time the situations are broader and more avoided anxiogens, which in turn strengthens the problem more and more, reaching extremes that neither alone nor accompanied can risk going out given the immense generalization that is being produced. Their anticipations are extreme and the disturbances they cause are very severe. Hence, it is essential to go to a qualified professional to help them solve such a highly disabling problem.
Both fears and phobias and consequently the anxiety that derives from it, will be overcome when people stop avoiding and face what they fear so much and can see for themselves, after multiple exposures, confrontations, different techniques and acquisition of sufficient resources and skills, that the consequences are not as dire as they thought and that what they so much they feared.
Therapies.
There are different techniques to deal effectively with these disorders, techniques that will be similar for both children and adults, although with small differences in the way of applying them, depending on the age or the characteristics of the problem, so it will be important to carry out a good functional analysis so that it allows to provide enough information about what is really happening in each case so that, based on this, to be able to act in the best way possible.
Among the most used techniques that are providing the best results when it comes to combating these problems, we can consider the following:
Psychoeducation: fundamental for the person to understand what is really happening, both at a cognitive, physiological and motor level, what is maintaining the problem and why, what can do to control the three levels of response... It is about providing the maximum relevant information related to both the phobic stimulus and the maintenance of the problem using for this, informational psychotherapies, bibliotherapy..., but above all an understandable language of the different concepts related to both the acquisition and maintenance of trouble.
Systematic desensitization: especially suitable for learning to respond without anxiety to stimuli that provoke inappropriate responses. Its objective is to face threatening situations gradually (both in imagination and in reality) using a previously established hierarchy of situations, associating all this with progressive relaxation and slow pulmonary and diaphragmatic breathing to counteract some emotions with others and get accustomed to situations threatening. It can be used in both children and adults as it allows us to elicit fear at will and confront ourselves in a graduated and controlled to the different stimuli that provide fear from lowest to highest degree of intensity based on the hierarchy of fears established.
Techniques for managing the anxiety that accompanies phobic disorders:(progressive muscle relaxation, slow diaphragmatic breathing, distraction, self-instruction, focus of attention ...) There are numerous relaxation techniques but Among them, the "Jacobson's progressive muscle relaxation" stands out both for its simplicity of application and for its high effectiveness in treating anxiety. The fundamental characteristic is that it allows generating, through the absence of tension, responses that are incompatible with the stressful activation of an organism. It makes it possible to clearly discriminate signals of tension in the different muscles of the body by learning systematic tension-relaxation exercises. The relaxation obtained at the muscular level automatically generates the relaxation of both the autonomic nervous system and the system central nervous system, which in turn enhances both cognitive and emotional relaxation, allowing you to perform without difficulties certain behaviors that interfere with those of flight, escape or avoidance, considerably increasing success in future clashes.
Exposure therapy both live and through images: causing behavioral experiments that allow progressively desensitizing the phobic element and eliminating little by little all the responses aimed at avoiding the feared situation both on a cognitive and physiological level and motor. In the exhibition we will use the exhibitions combined with relaxation techniques, self-instructions... to generate progressively habituation, satiety and desensitization through both live and image exposure to stimuli phobic. Its main objective will be to provoke emotional states incompatible with anxiety and with the phobic reaction. The duration and intervals of the exhibition will be adapted according to the responses that are obtained, increasing both as the confrontations are overcome.
Modeling techniques: very useful to solve phobias when used for therapeutic purposes because they allow, through the observation, learn from the adaptive behaviors performed by other people in order to modify theirs. They can be used with both children and adults, but it is children who can benefit the most from it. The observation of models can be done through drawings, films, real cases... The child observes another child how she copes with the situation feared, how it approaches, how it does it without anxiety and even how the model enjoys... From there, it is encouraged to carry out the behavior through relaxation, exposure and confrontation with the feared situation, supporting, encouraging and motivating him at all times until he gradually conquers his fear.
Emotional staging techniques: Like the previous one, very suitable for children because it combines relaxation, systematic desensitization, the participant, emotional pictures to inhibit anxiety (pictures that they can draw or create themselves) role play with exchange of roles, and something very important the positive reinforcement before any behavior of approach and confrontation to the feared object.
Cognitive-behavioral therapies: they are the therapies that are giving the best results. Cognitive-behavioral therapies combine cognitive restructuring procedures, relaxation-desensitization, training in resources and skills to be able to expose and cope with phobic stimuli, problem solving, self-instruction, control of thought... The rationale behind these therapies is to encourage people with these disorders to continually confront their catastrophic and highly negative beliefs with reality. eliminating avoidance from their repertoires and increasing exposures until they achieve desensitization that allows them to face and adapt to situations in a much more effective way realistic, adaptive and rational in such a way that they can be able to clearly discriminate what is really dangerous and what is the product of their imagination but does not represent any real danger.
Therapies based on virtual reality: Very useful to carry out expositions as many times as we want without having the phobic stimulus in front of us since all the therapy is carried out on a virtual level.

Recommendations.
FEAR APPEARS. WHAT NOT TO DO?
- Laugh at the reactions that the child presents.
- Allow others to laugh at him.
- Compare him with other children who don't present their fears.
- Criticize or punish you for being afraid.
- Make public your reactions and behaviors to fear.
- Insist with arguments and reasoning, continually reminding him of his fear of her.
- Force you in rude or authoritarian ways to deal with phobic stimuli.
- Threaten him with the stimulus he is afraid of ("if you don't eat the bad man will come", if you don't do this or that I will lock you in the dark room "...).
- Protect him excessively by avoiding any threatening stimulus or any confrontation with the phobic stimulus ...
FEAR APPEARS. TO DO?
- Act with the utmost calm when you present the fear response, or the "panic attack."
- Speak with low tones, rhythms and slow movements and as relaxed as possible.
- Give emotional support and, whenever possible, physical contact.
- Train the correct confrontational reactions through games and encourage him to play to check his progress.
- Let him face the little fears, get used to them on his own. Eg ocean waves, darkness, animals, noises ...
- Congratulate him on any progress in overcoming his fears, avoiding "tails" of the type: "it was about time that" "it was not so bad"... "
- Convince him that there is no need to be ashamed of being afraid of certain things. Use phrases like "I was also afraid of ..." "you are much braver than me"
- Offer correct models of how to act. Eg: riding on the swing, entering the dark ...
- Approaching the fear-provoking stimulus progressively, little by little and always in a pleasant and fun environment for the child
Attitudes that can prevent the appearance of phobias.
- It is important to test and contrast to what extent what one fears can have the consequences that one believes. The key for fears to appear is found in the immediate well-being that we obtain when we escape and avoid what we fear so much. By avoiding it, we prevent learning to control it.
- From education it is very important to teach a child to check whether something should or should not be feared: swimming pool, dogs, darkness, being or sleeping alone... it will make later, in adulthood, much easier to face other fears: death, heights, talking to others ...
- Have the child check through experience and in a graduated manner, what happens when she stays in the dark room, or what happens if she touches the bottom of the pool, or what happens if she touches a puppy... for example, it will help her to perceive that her surroundings should not be feared in excess. On the other hand, the fears of the parents, the search for guarantees that nothing will happen to the child, when they they exaggerate too much, it will not only make it enormously difficult to reduce the fears in the future but it will amplify them.
- Sometimes it is the parents themselves who transmit fears to our children by taking too many precautions derived from our own fears.
- It must also be specified that not everything that is feared must be overcome, after all, the feeling of fear, at first, is the adaptive response that our mind gives to favor the probability of survival.
- In other words, fears are necessary because they are often totally adaptive. The problem is when they cancel us out and block us without our being able to move forward or when they incapacitate us to lead a normal life, only then do we have to act.
- Use a positive education style, using educational techniques based on kindness, calm and respect for children, rather than using punishment and threats. Above all, physical punishment or psychological threat should not be used, there are other much more effective ways to educate.
- Avoid scaring the child even "as a joke", especially scares in the dark are contraindicated.
- Be attentive to what the child sees on television: You should not watch scary or violent movies that lead them to exaggerate fictitious and unreal situations in their imagination but which they assume as real.
- When the child cries at night because he is afraid, it is preferable to calm him in the dark and then, if anything, turn on the light, so that you never associate darkness with fear.
- Teach him to solve the little difficulties of daily life on his own. Do not give him things done or avoid the little frustrations with which he must necessarily face.
- Teach him to observe, see, and reinforce any courageous and confrontational behavior that he may have, however small or minimal it may initially seem to us.
- Don't use fear to control you: “if not, the bogeyman, the witch, the bogeyman will come... "
- Do not tell horror stories or tales, nor especially highlight or exaggerate the scariest aspects of traditional tales, always provide solutions and alternatives to solve problems.
- Read or have him read stories in which children like him overcome small fears or difficult situations, Make funny stories about those situations that may scare you and that he provides solutions and narrates alternative stories.
- If we are afraid of something we must learn to solve it, to keep control and to try to overcome our own fears so as not to transmit them to them, and thus be able to serve as role models in the face of our children's fears.
10 rules to deal with panic.
- START BY ACCEPTING FEARS. Accepting your fears and worries is the first step in getting rid of them. We should not feel ashamed or guilty for being afraid. If they are assumed and accepted, we will be able to talk about it and rationalize it.. The mere fact of counting things automatically makes them lose importance.
- REMEMBER THAT SENSATIONS ARE NOT MORE THAN AN EXAGERATION OF NORMAL BODY REACTIONS TO A PERCEIVED DANGER. They are not harmful or dangerous - just unpleasant. And above all, nothing worse can happen because in every anxiogenic process, everything that goes up goes down.
- WAIT AND GIVE TIME FOR THE FEAR LITTLE BY LITTLE TO DECREASE. Do not run away from it, simply accept it until we control the anxiety it generates but face it. Observe something fundamental and that is, as soon as we stop adding distressing thoughts fear will begin to fade on its own.
- CHANGE THE NEGATIVE THOUGHTS THAT USED TO ACCOMPANY THESE STATEMENTS FOR POSITIVE THOUGHTS. Do not add anxious thoughts about what is happening or what may happen to us to panic. It's very important learn to stop thinking when we detect that we are giving ourselves negative self-instructions ("I will not be able to", "this situation is horrible" "I can not" "I am very afraid" ...). At that moment inwardly shout "STOP!" And replace these messages with: Positive thoughts ("I'm going to get it", "the situation is difficult, but I'll be able to handle it" "I'm scared but if I face it, I'll stop having it" "I'm going to face it" "I'm going to try, I sure can" ...
- OBSERVE WHAT IS REALLY HAPPENING IN THE BODY RIGHT NOW, AT THIS MOMENT,JUSTWHEN THE PROBLEM IS BEGINNING In order to control the responses in the most relaxed way possible without making strange or catastrophic anticipations loaded with bad omens. It is also very important that instead of worrying let's do something fun such as, for example, thinking of something pleasant while facing off, doing something that we like (taking the bike, reading a comic, playing ...) will make worries forget. Exercising will also help us to be more relaxed and to release the tension accumulated by fear.
- WAIT AND GIVE TIME TO FEAR SO THAT LITTLE BY LITTLE IT WILL DECREASE. Do not run away from it or avoid it, simply learn to accept it until little by little we control it. Observe something fundamental and that is, as soon as we stop adding distressing thoughts fear will begin to fade on its own.
- LEARN RESOURCES AND SKILLS TO DEAL WITH FEAR, THE KEY BEING EXPOSURE, CONFRONTATION AND NON-AVOIDANCE - without avoiding it or running away - but taking advantage of the situation as an opportunity to practice, learn, advance and combat it. It is very important to learn to breathe deeply. When we are nervous we breathe very fast and shallow, because we only fill the upper part of the lungs. We can improve breathing by making it slow and deep. For this we fill the lungs slowly to the bottom, taking as much air through the nose, and then we also expel it slowly through the mouth. And at the same time we exhale the air, we can think for ex. how by expelling the air we eliminate with it the fears and the things that worry us.
- USE RELAXATION AS AN ESSENTIAL ELEMENT TO BE ABLE TO DEAL WITH PHBIC SITUATIONS.You cannot be scared and relaxed at the same time. If we learn to relax we can counteract the feelings of fear and help us to approach or overcome the feared situation. A very easy method of relaxing muscles is to focus on one part of the body (for example, the arm) and squeeze your hand firmly for a few seconds to feel the tension in the muscles of the arm; as soon as you stop squeezing you will notice the relief and the feeling of relaxation in your arm. You would have to repeat it once or twice and do the same with all parts of the body until you have mastered the technique.
- ALSO USE MENTAL IMAGES TO IMAGINE PLEASANT SCENES AT THE TIME THAT FEARS OR WORRIES ARE DISAPPEARED. If we already know how to breathe slowly and relax our muscles, we can try to imagine a pleasant scene that provides us with tranquility (eg, we are lying on a quiet beach, noticing the warmth of the sun's rays on our body, or we are traveling on top of a cloud, floating in the air, while the wind carries our fears ...)
- ALWAYS THINK ABOUT THE PROGRESS WE HAVE MADE DESPITE THE DIFFICULTIES. This will greatly strengthen us and make us feel very proud of our achievements, as well as providing us with increasing security.
- HELP US WITH SELF-RECORDS Writing the fears that we are facing, the strategies used to overcome them, or simply write what we say or should say to ourselves when we feel fear or worry. It will help us better understand what is happening to us, what we can do and how we can cope when it comes to overcoming fears. This technique provides many self-control strategies at all levels and can help us a lot to solve multiple problems.
- AS WE FEEL A LITTLE BETTER, LET'S LOOK AROUND OURSELVES AND PLAN THE NEXT STEP TO KEEP ADVANCING. We generally avoid thinking about our fears, because that way we feel more secure and we believe that this way we will feel better. But what if we did the opposite? We can test to see what happens and plan the next steps to move forward and desensitize. We also discovered that those fears no longer scare us as much as we thought, or it is simply possible that we manage to see the situation in a very different way than we thought.
- WHEN WE ARE PREPARED TO CONTINUE, LET'S START AGAIN IN A QUIET AND RELAXED WAY. There is no need to run, let's do it little by little, little by little, moving forward but without stopping and the more we repeat the little ones progress much better because the more we will consolidate the results and the better we will learn to solve the next challenges and thus overcome the fears.

Final reflection.
IT IS ALWAYS BETTER TO PREVENT THAN TO CURE: sometimes we can avoid situations that cause us fear. For example, a child who is afraid of nightmares should not watch movies before going to bed that may scare them, nor should they eat large meals or very strong and indigestible that can cause discomfort that could lead to conditioned fears or drink caffeinated drinks or any other substance exciting. Why provoke a situation without first being prepared to resolve it?
And something very important!
In the face of fears, never avoid because with avoidance the fear will grow, spread and generalize to many other situations, for Although it generates some anxiety, it is much better to expose yourself, face it, solve it and analyze the consequences that avoid it. The anxiety that it can generate when trying to solve it will always be much less than the problems generated by its maintenance.
This article is merely informative, in Psychology-Online we do not have the power to make a diagnosis or recommend a treatment. We invite you to go to a psychologist to treat your particular case.
If you want to read more articles similar to Fears, Anxiety and Phobias: differences, normality or pathology?, we recommend that you enter our category of Emotional and behavioral disorders.
Bibliography
- Antony, M.A. and Barlow, D.H. (1997). Specific phobia. To see. Horse (Dir.), Manual for the cognitive-behavioral treatment of psychological disorders (Vol. 1, pp. 3-24). Madrid: XXI century.
- Ayuso, J.L. (1988). Panic disorders. Barcelona: Martínez Roca.
- APA. (2002) “Diagnostic and statistical manual of mental disorders. DSM-IV-TR ". Editorial Masson.
- Bados, A. (1998). Specific phobias. In Vallejo, M.A. (Ed.), Behavior therapy manual, (Vol I, P. 169-218). Madrid: Dykinson.
- Bados, A. (2000). Agoraphobia and Panic Attacks: A Step-by-Step Psychological Intervention Program. Madrid: Pyramid.
- Bados, A. and Coronas, M. (2005). Intervention in a case of blood / injection / wound phobia (pp. 47-65). In J.P. Espada, J. Olivares and F.X. Mendez (Coords.), Psychological therapy: practical cases. Madrid: Pyramid.
- Bados, A. and Guardia, J. (1983). Elimination of various animal phobias by participant modeling, using a multiple baseline design. Spanish Journal of Behavior Therapy, 1, 143-160.
- Ballesteros, S. General Psychology II. A cognitive approach. (1994). Madrid: Editorial Universitas S.A.
- Bastida de Miguel, A.Mª. Psychotherapy applied to a case of night terrors with generalized anxiety caused by a multitude of phobias.12th Virtual Congress of Psychiatry (6conf1550204). Interpsiquis - February-March 2011. Psychiatry.com
- Bastida de Miguel, A.Mª. Cognitive-behavioral treatment in a case of obsessive disorder-compulsive. 10th Virtual Congress of Psychiatry. Interpsiquis - February 2009. Psychiatry.com Y Psychology. International On-line Journal of Psychology - ISSN 1137-8492 (Vol.13 Nº1-Jan 2009)
- Beck, A, and Freeman, A. Cognitive therapy of personality disorders. Paidos. 1995
- Belloch, A.; Sandín, B. and Ramos, F. Psychopathology Manual. Vol. II. (2.002). Madrid. McGraw-Hill Interamericana of Spain.
- Bernstein, D. A., Borkovec, T. D., Progressive Relaxation Training. Bilbao, Desclee, 1983
- Bottle, C. (2001). Effective psychological treatments for panic disorder. Psicothema, 13, 465-478.
- Bottle, C. and Ballester, R. (1997). Panic Disorder: Evaluation and Treatment. Barcelona: Martínez Roca. Fob Esp - 65
- Bottle, C., Baños, R.M. and Perpiñá, C. (Comp.). (2003). Social phobia. Barcelona: Paidós.
- Bragado, M.C. (1994). Behavior Therapy in Childhood: Anxiety Disorders. Madrid: University-Business Foundation.
- Bragado, M.C., Carrasco, I., Sánchez, M.L. and Bersabé, R.M. (nineteen ninety six). Anxiety disorders in schoolchildren aged 6 to 17 years. Anxiety and Stress, 2, 97-112.
- Horse, V.E. and Simón, M.A. (2002). Child and adolescent clinical psychology manual. General disorders. Madrid: Pyramid.
- Capafons Bonet, J. I. (2001). Effective psychological treatments for specific phobias. Psicothema, 13, 447-452.
- Echeburúa, E. (1993c). Anxiety disorders in childhood. Madrid: Pyramid.
- Eysenck, M. W., and Derakshan, N. (1997). A cognitive theoretical framework for anxiety disorders. Anxiety and Stress, 3, 121-134.
- Freem.
Photos of Fears, Anxiety and Phobias: differences, normality or pathology?