
Cancer or neoplastic disease is the second cause of death in Cuba and in the world. Worldwide the oncohematologic disease in children, 16 cases are diagnosed for every 10,000 children under 15 years of age. The approximate mortality in general is 3.6 to 3.8 per 100,000 inhabitants. In Cuba, pediatric cancer constitutes only 2% of malignant tumors, but it is the leading cause of death from disease in children under 15 years of age. In our country, around 300 new patients with malignant neoplasms are diagnosed each year in children under 18 years of age.
Index
- Comprehensive Program for Cancer Control in Cuba
- Resilience in childhood cancer cases
- Material and method
- Ethical aspects
- Results
- Protective factors of family resilience
- Family risk factors
- Discussion
- Protective factors
- Family risk factors
- Intervention program
- Intervention proposal
Comprehensive Program for Cancer Control in Cuba.
Due to the threat posed by cancer to the world population, it became essential to create and implementation of the Comprehensive Program for Cancer Control in Cuba, which has as its purpose
This program includes a strategy for the control of childhood and adolescent cancer and the essential involvement of Primary Health Care in the timely diagnosis from the surveillance of risk factors, symptoms and warning signs and in the process of follow-up and rehabilitation biopsychosocial.
The cancer diagnosis in a child it produces an important socio-emotional impact on the whole family. The sick child and her family will have to face diverse and difficult events that can hinder the future of their lives. It could be considered as a crisis, given the disorganization that occurs and that impacts each of its members.
To adapt to this situation, the family sets up self-regulation mechanisms that allows it to continue to function, in such a way that changes are generated in family interactions that have a specific purpose, conscious or unconscious, and that can lead the family to complex situations of balance or imbalance, putting the well-being and management of the sick patient at risk, as well as the functionality of the system familiar.4
Resilience in childhood cancer cases.
This investigation was made necessary and relevant from a social point of view, Since it was aimed at a vulnerable sector of the population, this disease being a stigmatizing pathology that encompasses many negative feelings for those who suffer from it and those around them. This is a problem that has also currently acquired great social magnitude, thus becoming the work with patients pediatric oncopaediatrics a priority of the Cuban National Health System, as well as the timely intervention of Primary Health Care in assisting these children.
The research responded to the objectives of the Cancer Control Program in Primary Care, specifically from the consideration of the problem within the problem bank of the Polyclinic, also being the first investigation that addressed Pediatric Psycho-Oncology from Primary Health Care in the municipality. This research studied a topic that turns out to be interesting and novel, since family resilience has been poorly addressed internationally and in the country, in addition to its limited treatment linked to oncohematological diseases, which accounts for the lack of antecedents in this regard.
The research has a practical projection, since it tried to form a methodological guide for the therapeutic approach of said problem, allowing the development of the resilience capacity in these families, which became opportune due to the lack that from Psychooncology and family studies, there were interventions with such purpose.
Due to all of the above, the investigation was drawn as the main question: How develop resilience capacity in families with children with oncohematological diseases health area of the Pedro Borrás Polyclinic?, also pursuing the general objective: Design an intervention program to develop resilience capacity in families with children with oncohematological diseases in the Pedro Polyclinic health area You will erase.

Material and method.
The specific objectives pursued are:
- Describe the resilience capacity of the study families.
- Plan the intervention program proposal.
The present investigation constituted a non-experimental, descriptive, cross-sectional study, which responded to a mixed design in parallel, carried out in the period between September 2011 and April 2012.
The study universe was made up of the 4 families with children with oncohematological diseases belonging to the health area of the Pedro Borrás Polyclinic. The study sample was non-probabilistic of typical subjects, made up of the 4 families, which was selected by the following criteria:
Inclusion criteria
Families willing to participate in the study.
Exclusion criteria
- People within the family nucleus who present a mental, auditory, verbal and visual disability that prevents them from participating in the study.
- Children five years of age or younger, whose intellectual maturity would not allow them to answer the data collection techniques.
- Older adults with a mental capacity that did not allow them to understand and respond to the techniques used.
Evaluation instruments
To collect the information, the following evaluation instruments were used:
- Family interview
- Family resilience questionnaire
- Family risk factors questionnaire
- Family Cohesion and Adaptability Assessment Scale (FACES III)
- Rating scale
- Family shield
- Family circle method
- Family drawing
- Composition
These last two techniques were applied only to children with the disease, taking into account the application peculiarities for the age periods, while the other techniques were applied to the members remaining.
For information processing data triangulation was used, from the integration of qualitative and quantitative data, in addition to being based on categories previously established and others constructed by the researcher from the discourse of the subjects of the study. In the same way, descriptive statistics were used, through the recording of frequencies, which were presented in texts and tables.
Ethical aspects.
This research was carried out taking into account ethical principles such as I respect people from the treatment of subjects as autonomous beings, respecting their opinions and criteria, as well as their willingness to participate in the study, through the use of informed consent as part of the process of accessing the sample of the study.
The information obtained in the research was used strictly for scientific purposes, presenting its results, without revealing the identity of the subjects. In addition, the principles of beneficence, non-maleficence and the principle of justice.

Results.
The resilience manifested by the study families was characterized by the presence of a minimal resilience approach. This was sustained on the basis of passive adaptation to the crisis experienced, based on the maintenance and emergence of irregularities in family functioning, present in protective factors of resilience and the identification of factors of risk.
Protective factors of family resilience.
In the case of family beliefs as part of the subjective structuring of the situation, they moved in correspondence to the different moments of the illness, the concrete situations experienced by the families and the meaning they were having for them. The presence of beliefs centered on the negative aspect of the event was shown during the stages of diagnosis and hospitalization in 100% of the patients. cases, as well as the beliefs aimed at mitigating the negative connotation of the event after the end of the hospital treatment and in the present. Beliefs aimed at giving meaning to adversity were not shown in any of the cases.
100% of the cases maintained a negative evaluation of the event during the diagnostic and hospitalization stages, while the treatment is finished hospital and currently, 50% of the sample held a positive evaluation of the crisis in question. The future perspective of 100% of the families was pessimistic during the diagnosis and hospitalization, however this was modified, also in the entire sample, to an optimistic position during the period of completion of hospitalization and in the present. The entire study sample (100%) suffered from the presence of faith and spirituality to face the family crisis during the time of diagnosis and hospitalization, while hospital treatment ended and at present, this factor was present in 75% of patients. cases.
With respect to family communicationr The absence of indicators such as clarity and the sincere expression of feelings around the family crisis experienced was evidenced in 100% of the families in the study.
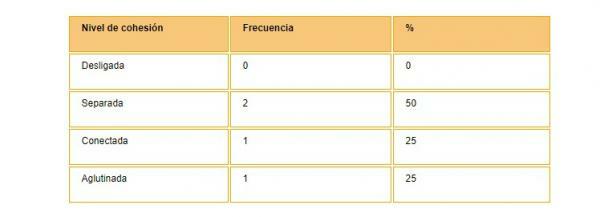
Regarding the behavior of family cohesion in the face of the crisis (image) the predominance of separated families was shown in the cases studied, an intermediate category within family cohesion from Olson's circumplex model. The absence of unrelated families was also evidenced.
The behavior of the family flexibility was characterized by the predominance of structured families, where 50% of the families were located in this category, which is one of the intermediate ones within the family flexibility from the circu-complex model of Olson. The absence of families with a level of chaotic flexibility was also shown
Family risk factors.
The presence of family problems between the different subsystems in 50% of the cases.
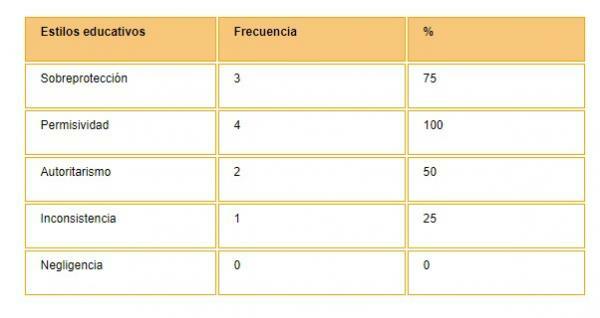
Among the inappropriate educational styles used more frequently by the families in the study, (Table 2) the permissiveness and overprotection. The absence of negligence as an educational method was also shown.
As part of the ineffectiveness in the exercise of roles in the face of the family crisis, the predominance of the presence of overload and rigidity was manifested in 100% of the study cases.
Within the para-normative family crises, a predominance of the crisis was evidenced by increase and by dismemberment, which were present in 3 of the cases, for 75% of the sample of the study. The absence of a crisis due to disorganization was also shown in the face of the situation experienced.
Discussion.
Taking into account the existence of family resilience from a minimum approach, it is important to highlight the variability in the behavior provider of resilience of the protective factors in the study families, while difficulties were manifested in the resilient involvement by some of the these. In relation to family risk factors, it was shown the neutralizing action of these.
Protective factors.
The family belief system in the face of the crisis experienced did not constitute a protective factor of resilience. No beliefs aimed at giving meaning to adversity were shown, while the beliefs did not imply the rearrangement of meanings from the intention of giving coherence to the event, and visualizing it from constructions that allow it to be assumed as part of reality family.
The evaluation of the event from negative implications and connotations was maintained in 2 of the studied families for the family system, preventing this from being viewed as a challenge or opportunity for growth family. The presence of negative future prospects was an impediment to a belief system of family resilience. Only the presence of faith and spirituality after the end of the hospitalization period was favorable to a resilient belief system, being assumed as a source of comfort and family strength in the face of the crisis experienced
Family communication did not contribute to the development of resilience, while the difficulty in expressing feelings generated by the situation and the lack of clarity, given by the failure to communicate the diagnosis to the patients. children with the disease, hindered family communication, since the subject was a family secret and did not allow the free emotional exchange of messages.
The Leukemia and Lymphoma Society supports the negative effects produced by silence around the situation, inasmuch as it suggests that children who are not informed or not given the opportunity to ask about their illness, far from being protected from fear and worry, they may come to think that illness is a taboo or a dangerous secret Not to talk about and develop scary fantasies and fears about what is happening to you.
The existing difficulties in relation to clarity, manifested in the presence of guilty messages, messages with double meanings, and directionality masked, bringing with it the expression of family conflicts, and their inadequate channeling, also negatively affected the resilient behavior of this factor.
The predominance in the studied sample of separated families diverges with those revealed by the research “Styles of family relationships and resilience in families of cancer children ”, in which the predominance of amalgamated families was observed, representing 28% of the sample of the study.6
Even when certain irregularities were manifested in this factor in the family system as a whole, it was considered as an important source of the Resilience manifested in the families of the research, while taking into account the implication of the autonomy that this quality must provide to the members. Hence the importance of this factor in the presence of a crisis, element that is endorsed by Walsh from the opportune interventions of him, insofar as he states that the capacity for family reorganization after the crisis is based on family connection, and implies a balance between unity, mutual support and collaboration on the one hand, and the separation and autonomy of each individual on the one hand other.7
The predominance of structured families is congruent with the results obtained in the research “Styles of family relationships and resilience in families of cancer children ”, where 30% of these were located in said category.
Even when this level of flexibility allowed an accommodation and restructuring of the family reality, the susceptibility of this to be molded was evidenced.
Family risk factors.
The existence of family conflicts cIt agrees with the proposals made by Martínez V and Real G, who endorse a high frequency of conflicts derived from the illness, altered marital relationships, marital problems, sexual dysfunctions, and separations and divorces.6
The predominance of permissiveness as an inappropriate educational style is understandable and valid in light of statements made by Patricia Arés, who states that the Permissiveness can appear in contexts where adults feel sorry for their children for some illness or painful situation experienced by east.8
Precisions made by Grau C and Fernández M, agree in conceiving of overprotection as a risk factor within inappropriate educational methods, since they consider that the overprotected child may realize that she occupies a privileged place in the family, which confirms his feelings of fragility and anxiety regarding her survival .9
The predominance of overprotection as an educational style Faced with the crisis experienced, it agrees with the results specified in most of the Psycho-oncology and family studies, where the establishment of psychopathogenic attitudes of overprotection or greater rigidity and less flexibility than in parents with adolescents without cancer.10
The absence of negligent styles in the sample studied also accounted for the social significance that underlies the illness and the urgent need to fully comply with the behavioral demands proposed by the staff doctor. These results are congruent with those obtained in the research "Living with a child's cancer", where the majority of mothers and Parents understood that they should be even more diligent and careful in following the treatment even if the child did not show signs of the disease.11
Although ineffectiveness in the exercise of roles did not negatively influence as a determinant of family resilience capacity, it is an element susceptible to modification and refinement, since overload was shown in the maternal figure, promoting physical wear and tear and emotional. In addition to the rigidity in the roles, the dichotomous distribution of the tasks in the situation and in correspondence with the traditional sexual stereotype manifested.
The presence of dismemberment crisis, given by the divorce of the parents and their inadequate management, constituted a hindering factor of a better development of intra-family relationships for positive coping with the crisis experienced.
The results revealed in the investigation showed the essential psychological intervention in this regard. Also, considering that resilience is neither absolutely nor permanently stable, it is important professional performance anticipating the occurrence of subsequent situations that destabilize the family.
Intervention program.
The design of the intervention program was aimed, essentially, the development of resilient family characteristics and action on those risk factors identified in families.
The program will be aimed at the cohabitation family of the child with the disease, rescuing the father figure in cases where it does not live with the child. Children with the disease and other children in the family will be excluded.
The program includes 13 work sessions, including the intermediate and final evaluation session. It is planned to be carried out, executing each session on a weekly basis, so the duration of the execution should be 3 months and a week. Each session lasts from 20 to 55 minutes. The place where the sessions will take place will be in the Psychology consultation and the executors will be the psychologists of the GBT (Basic Work Group) and the Psychologist of the Functional Control Group of Cancer.
The program will be carried out through therapeutic groups, where health education will be combined with group therapy, relying on participatory techniques that constitute tools within the educational process, and those of psychodrama, as a therapeutic procedure for the representations of the different roles in the group. The objective of combining these techniques is to facilitate the process of internalization and rational elaboration from the experience.
The work sessions will be structured in three moments, a moment of beginning, a moment of development of the proposed objectives and the closing of the session. In addition, relaxation techniques will be used during the work sessions as part of the warm-up or the beginning of these, but that It is also intended that they be learned and put into practice in the daily family life in which stress is Present.
It will be carried out throughout the process, the collection of extraverbal information from the use of observation of the behaviors of the participants in group work, as another of the scientific methods of obtaining information. Will be lent special care and treatment, in addition, to aspects inherent to the development of the group, such as:
- Group homeostasis
- Presence of multiple transfers
- Reactive associations between members
- Defense mechanisms
- Activity sabotage as a form of avoidance
- Emotional contagion
- Group fragmentation
- Emotional reactions to the topic to be addressed
- Attacks on the coordinator
The evaluation of the program will be carried out through a midterm evaluation, after 6 sessions developed, an evaluation at the end of the program and another evaluation 6 months after the completion of this, through the re-test technique, applying again the instruments used to collect the information.
At the end of the program, the participants will be given a diploma that accredits them as resilient families, as a way of stimulating the group work carried out.
Intervention proposal.
General Objective: To develop the resilience capacity in families with children with oncohematological diseases.
Specific objectives
- Develop the granting of a sense of coherence to difficult situations.
- Develop the visualization of crisis situations as a way of family growth.
- Develop awareness of the importance of family cohesion in crisis situations.
- Train the ability to be flexible in situations demanding modifications.
- Train the open and sincere expression of feelings in situations with strong emotional charges.
- Emphasize the importance of an active family posture in difficult situations.
- Provide viable strategies for the adequate channeling of intra-family conflicts.
- Train empathic capacity among family members.
- Provide information about the harmful effects of inappropriate educational styles on children's behavior.
- Provide information about the main family roles, as well as their adequate assumption in crisis situations.
- Develop better family communication based on clarity.
- Develop the demonstration of affective correspondence in families.
This article is merely informative, in Psychology-Online we do not have the power to make a diagnosis or recommend a treatment. We invite you to go to a psychologist to treat your particular case.
If you want to read more articles similar to Children with oncohematological diseases and their relationship with their families, we recommend that you enter our category of Social psychology.
Bibliography
- Pérez NC. Characterization of the neoplastic disease of childhood in the province of Ciego de Ávila. Mediciego Magazine. [Internet]. 2010 [cited 2011 Oct 15]; 16 (1): [approx. 1 p.]. Available in: http://www.bvs.sld.cu/revistas/mciego/vol16_01_10/articulos/t-4.html
- Ministry of Public Health. Statistical Yearbook of Health 2010 [Internet]. Havana: National Directorate of Medical Records and Health Statistics; 2010 [cited 2011 Dec 18]. Available in: http://www.infomed.sld.cu/servicios/estadisticas/
- Ministry of Public Health. Comprehensive Program for Cancer Control in Cuba. Havana: Medical Sciences Editorial; 2010.
- Llorens A, Mirapeix R, López-Fando T. Siblings of children with cancer: result of a psychotherapeutic intervention. Psychooncology. [Internet]. 2009 [cited 2011 Sep 26]; 6 (2-3): [approx. 1 p.]. Available in: http://revistas.ucm.es/index.php/PSIC/article/viewFile/PSIC0909220469A/15207
- Torres Pardo B. Psychological impact of leukemia on the child and the family: coping strategies. Psiquiatría.com [Internet]. 2008 [cited 2011 Nov 22]; 6 (2): [approx. 1 p.]. Available in: http://www.psiquiatria.com/bibliopsiquis/handle/10401/4503
- Rodríguez VM, Real G. Styles of Family Relationships and Resilience in Families of Cancer Children and Adolescents. Journal of Psychology UAC. [Internet]. 2007 [cited 2011 Oct 12]; 3 (5): [approx. 1 p.]. Available in: http://www.monografias.com/trabajos-pdf/relaciones-familiares-ninos-oncologicos/relaciones-familiares-ninos-oncologicos.shtml
- Kotliarenco MA, Gómez E. Family Resilience: a research and intervention approach with multi-problem families. Journal of Psychology [Internet]. 2010 [cited 2011 Sep 22]; 19 (2): [approx. 1 p.]. Available in: http://www.tecnovet.uchile.cl/index.php/RDP/article/viewArticle/17112
- Arés P. The family. A look from Psychology. Havana: Scientific-Technical Editorial; 2010.
- Grau C and Fernández M. Family and pediatric chronic disease. Anales Sis San Navarra Magazine [Internet]. 2010 May-Aug [cited 2011 Sep 15]; 33 (2): [approx. 1 p.]. Available in: http://scielo.isciii.es/scielo.php? script = sci_arttext & pid = S1137-6272010000300008 & lng = es.
- EM War. Psychological characterization of adolescents with Acute Lymphoblastic Leukemia. [thesis]. Pinar del Río: University of Medical Sciences; 2010.
- Castillo E, Chelsa CA. Living with a child's cancer. Medical Journal of Colombia [Internet]. 2003 [cited 2011 Nov 10]; 34 (3): [approx. 1 p.]. Available in: http://redalyc.uaemex.mx/redalyc/pdf/283/28334308.pdf


